Student Led Research
A collection of research submitted by healthcare students. Each research submission has been edited by local experts.
Rare Variant of a Supernumerary Pectoralis Minor: A Case Report
Sarah Snyder, P.T., D.P.T.
University of Houston–Tilman J. Fertitta Family College of Medicine
Key Words: Pectoralis minor, pectoralis quartus, shoulder, musculoskeletal, anatomy, dissection
The author has no funding/grants to disclose for the completion of this work.
Summary
In the superficial chest wall, deep to the pectoralis major, one can find a thin, triangularly shaped muscle known as the pectoralis minor. It forms the anterior wall of the axilla and is frequently credited as a potential source for shoulder pathology. In the late 1800’s, anatomists had concluded that variants in pectoralis minor origin and insertion existed in up to 28% of the general population.1 A modern-day systematic review of 25 studies resulted in an aberrant insertion of the pectoralis minor muscle in 19.27% of individuals (95% CI 15-24%).2 During a dissection in an Anatomy Distinction Program led by Dr. Thomas Gest at the Tilman J. Fertitta Family College of Medicine, the author uncovered a particularly unusual variation that was noted within the body of an elderly female. Her right shoulder contained two different pectoralis minor muscles—one with the traditionally documented variation, and one with its own particular origin and insertion. The implications of such a variation are relevant to modern day treatment of orthopedic shoulder injuries as well as surgeries in the local region.
Case Presentation
Traditionally, the pectoralis minor muscle originates from the anterior surfaces of the 3rd, 4th, and 5th ribs near their costochondral junctions and inserts at the coracoid process of the scapula.3 This origin and insertion allow for the muscle to stabilize the shoulder as well as depress, internally rotate, and anteriorly rotate the scapula. With the scapula stabilized, it can also assist with elevating the ribs, functioning as an accessory respiratory muscle. More importantly, the pectoralis minor also functions as a bridge covering the brachial plexus, subclavian artery, and subclavian vein. It receives its innervation from the medial pectoral nerve (C8, T1) and may also receive partial innervation from a branch of the lateral pectoral nerve called the ansa pectoralis.3,4 Functionally, a shortened pectoralis minor muscle has been regarded as the source of poor “rounded” shoulder posture, leading to limited shoulder mobility as well as potential thoracic outlet syndrome.5 Studies regarding the variation in the anatomical position of the pectoralis minor traditionally mention unique sites of insertion. One famous 1897 study performed by Le Double documents what he would call a type I, type II, or type III variation of insertion, with insertion to the glenohumeral joint capsule being the most frequently documented unique site of insertion.
- Type I: A superficial portion of the pectoralis minor tendon continues past the coracoid process to attach to a more proximal location.
- Type II: Most fibers of the pectoralis minor tendon attach to the coracoid process and only a few continue over it.
- Type III: Entire the ligament passes over the coracoid to attach to a more proximal location and can be separated from the coracoid process by a bursa.
Le Double also documented various instances where the pectoralis minor muscle originated from as superiorly as the first rib to as inferiorly as the sixth rib.1 With an appreciation of embryology, it is possible to speculate at which period of development endogenous or exogenous factors may have contributed to each variation. Certain anatomists have speculated that there may be accessory pectoral muscles present as vestigial structures, evidence of human evolution from apes, which traditionally have four to seven rib attachments for the pectoralis minor muscle. Such accessory structures have been given names, and if we are to follow this theorem, this case study may present an example of a pectoralis quartus, “which runs from the lower ribs to various structures of the distal shoulder.”1 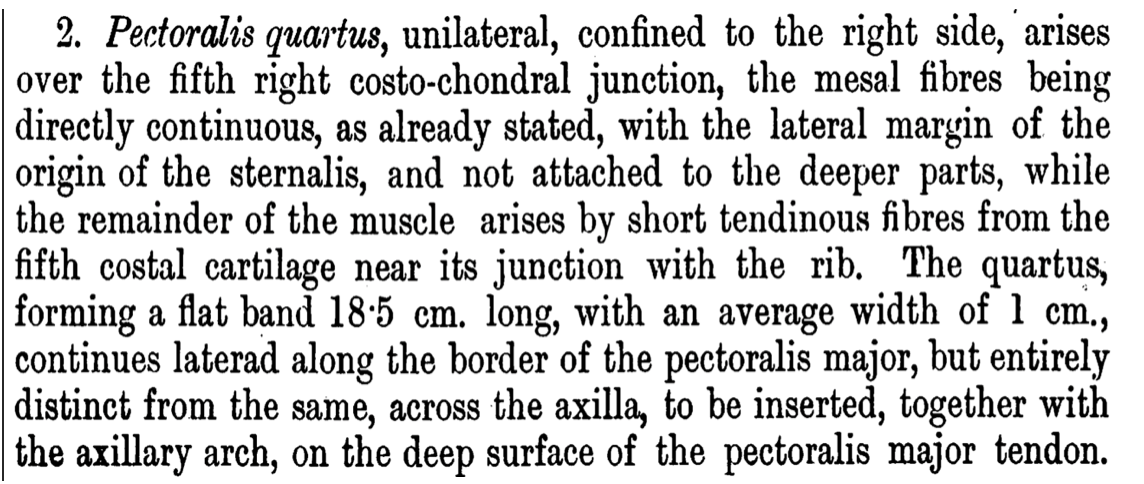
Fig. (1) An excerpt from “The Derivation and Significance of certain Supernumerary Muscles of the Pectoral Region,” authored by Dr. George Sumner Huntington, MD, professor and anatomist at Columbia University College of Physicians and Surgeons in the late 1800’s.6
Materials and Methods
The cadaver in question was obtained ethically via human body donation for the purpose of medical education. During the summer between the first and second year of medical school, students at Tilman J. Fertitta College of Medicine can apply to an Anatomy Distinction Program that involves six weeks of immersive dissection and practical examination. With deep reverence for the cadaver donated, an elderly female, the author performed routine medical dissection and noted all unique anatomical variations. All tissue was properly preserved and disposed of with respect to the donor’s body as well as the families of the individual.
Results
In the subject of study, the supernumerary pectoralis minor muscle originates from ribs six and seven and insert directly into the conjoint tendon— the tendon where the short head of biceps brachii and coracobrachialis muscles merge to connect to the fascia covering the apex of the coracoid process.2,3 This is lateral to where the pectoralis minor attaches to the superior and most medial aspect of the coracoid process (so named as it is derived from the Greek term for “raven” as its shape is hooked and resembles a large beak).7 The left pectoralis minor exhibits normal anatomy.
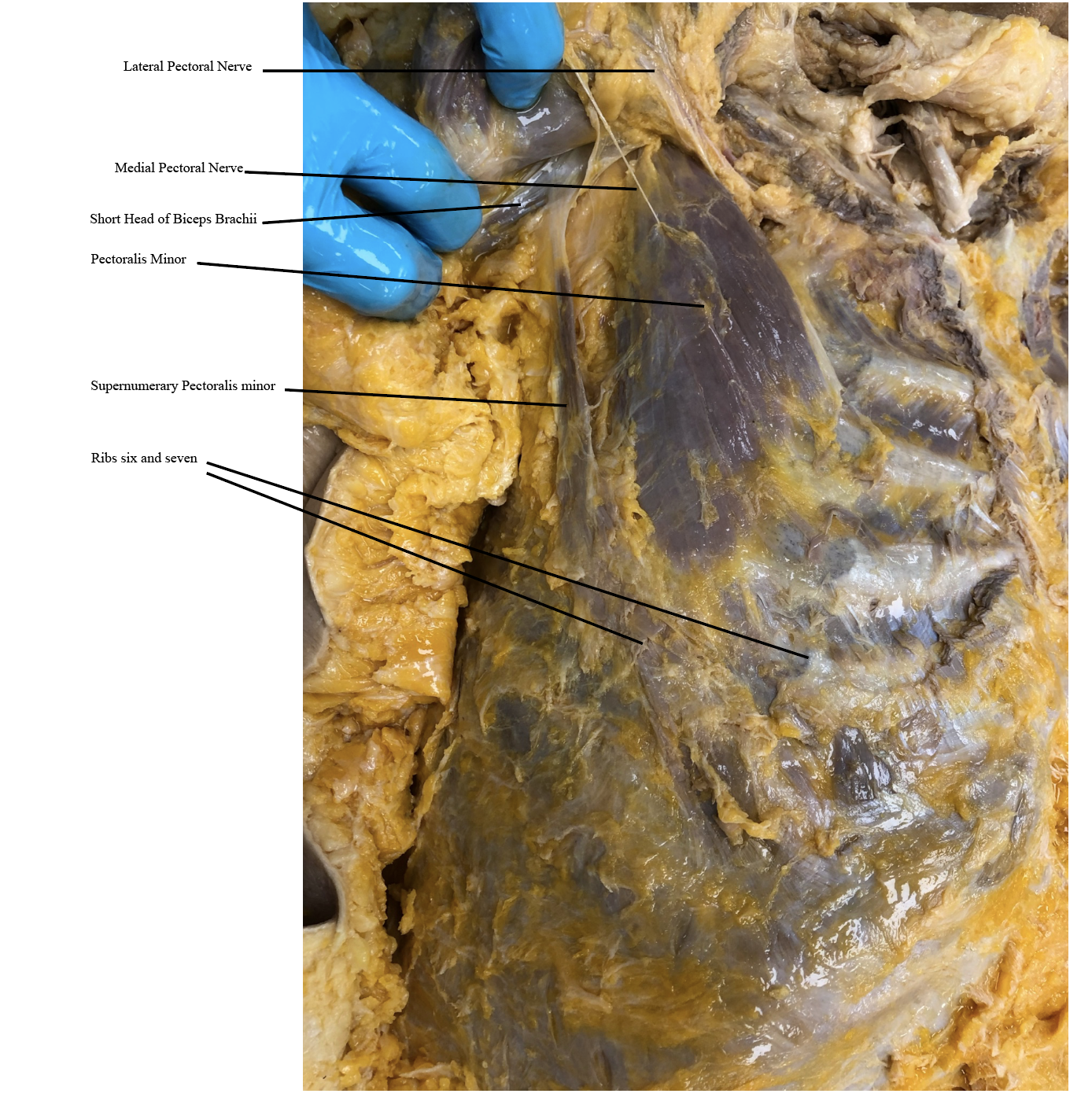
Fig. (2) Photograph of right anterior chest, displaying pectoralis muscle originating from ribs 6-7 and inserting onto conjoint tendon.
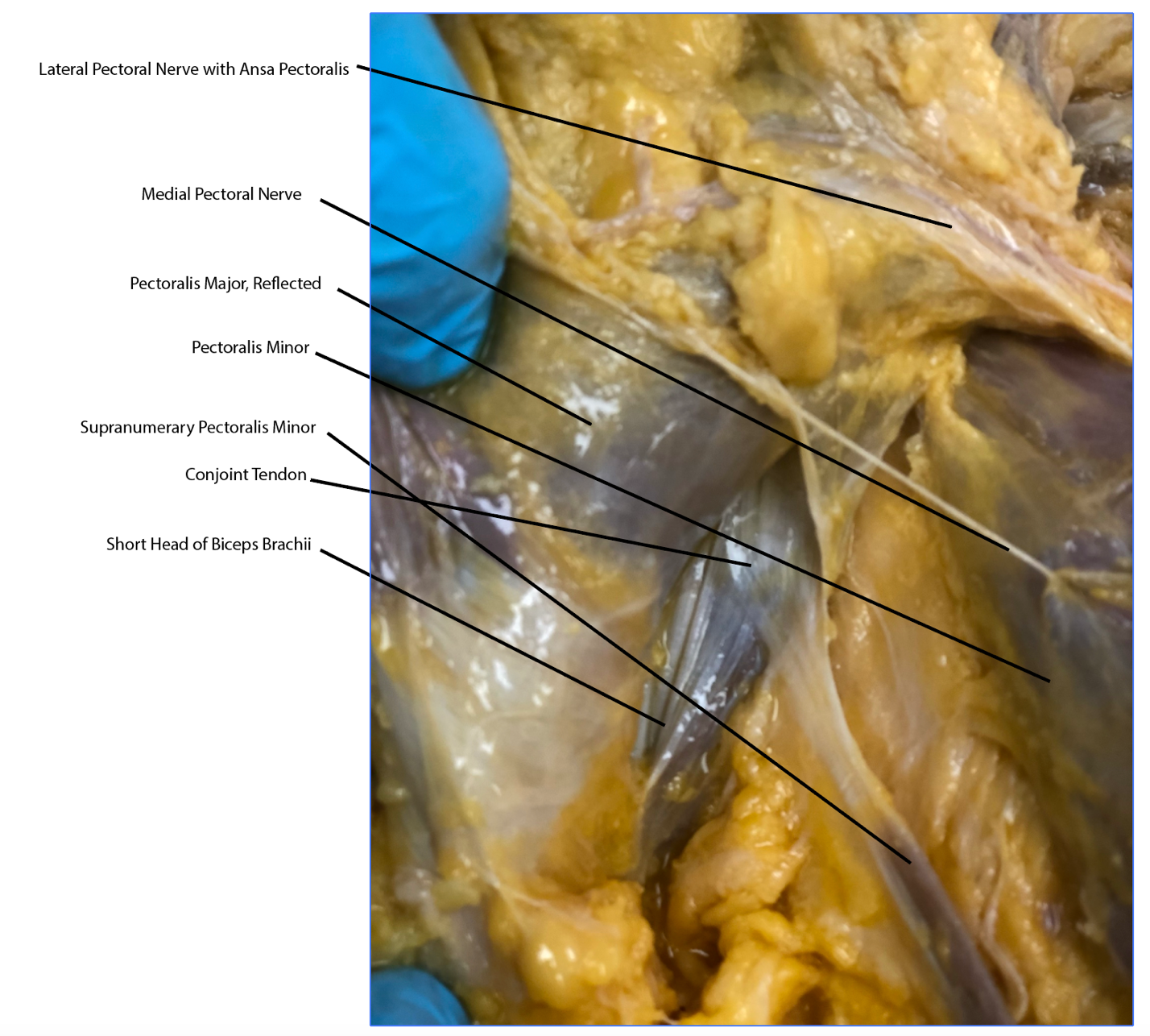
Fig. (3) Visual of insertion onto conjoint tendon.
Discussion
The study of the superficial musculature of the anterior chest wall can provide much insight regarding the pathology of the shoulder joint. Clinicians frequently struggle with the treatment of shoulder pathology as it is considered four separate true joints in one, making it the most mobile joint of the body. The high incidence rate of variations in the pectoral musculature can provide some insight regarding why certain individuals may be more prone to shoulder injury and instability than others. For example, for unknown reasons, the incidence rate of aberrant pectoralis minor muscles is significantly greater in females and prefers a left laterality — findings supported by four separate research studies.3 This unique case allows for the speculation of underrepresented and underreported anatomical variations within the general human population, emphasizing the importance for tailored therapeutic and surgical treatment or intervention of the area. In multiple ways, this is of surgical relevance as the pectoralis minor muscle is frequently utilized as a donor site for several reconstructive surgeries, including mandibular reconstruction.8 The pectoralis minor muscle is also used as a landmark for several structures, including lymph nodes. It is utilized to classify between zones I, II, and III axillary lymph nodes during a lymph node resection or mastectomy.9 Although there is no clarity regarding the innervation of the supernumerary pectoralis minor muscle, it provides a unique force vector onto the conjoint tendon. A dual innervation to the conjoint tendon (e.g., musculocutaneous nerve to the coracobrachialis muscle, and separate innervation to the supernumerary pectoralis minor muscle) would provide suspicion for impaired glenohumeral rhythm with mobility. Without knowing the medical history of the body donor, there can be no conclusions drawn regarding her right shoulder mobility in comparison to her left, and shoulder pathology regarding unique variations of the pectoralis musculature should remain a topic of interest to the orthopedic community.
Acknowledgements
The author was greatly supported by the wisdom, knowledge, and encouragement of
Dr. Thomas Gest, PhD, president of the American Association of Clinical Anatomists. It was Dr. Gest’s mentorship and deep reverence for the study of clinical anatomy that allowed this case study to come to fruition.
"The author[s] sincerely thank[s] those who donated their bodies to science so that anatomical research and teaching could be performed. Results from such research can potentially increase scientific knowledge and can improve patient care. Therefore, these donors and their families deserve our highest respect."10
References
1. Le Double A-F. Traité des variations du système musculaire de l'homme et de Leur signification au point de Vue de l'anthropologie zoologique. 1897. doi:10.5962/bhl.title.44649
2. Asghar A, Naaz S, Naya S. The prevalence and distribution of the variants of pectoralis minor in cadaveric studies: A systematic review and meta-analysis of 32 observational studies. Natl J Clin Anat. 2021(10):103-112. doi:10.4103/njca.njca_61_20
3. Asghar A, Narayan RK, Satyam A, Naaz S. Prevalence of anomalous or ectopic insertion of pectoralis minor: A systematic review and meta-analysis of 4146 shoulders. Surg Radiol Anat. 2020;43(5):631-643. doi:10.1007/s00276-020-02610-8
4. Netter FH. Atlas of Human Anatomy. Philadelphia, PA: Saunders/Elsevier; 2014.
5. Lee JH. The effect of scapular posterior tilt exercise, pectoralis minor stretching, and shoulder brace on scapular alignment and muscles activity in subjects with round-shoulder posture. J Electromyogr Kinesiol. 2015;25(1):107-14. doi: 10.1016/j.jelekin.2014.10.010
6. Huntington GS. The derivation and significance of certain supernumerary muscles of the pectoral region. J Anat Physiol. 1904;39(Pt 1):1-54.27. PMCID: PMC1287399
7. Liddell HG, Scott R. A Lexicon: Abridged from Liddell and Scott's Greek-English Lexicon. Oxford: Clarendon Press; 1993.
8. Burley HE, Haładaj R, Olewnik Ł, Georgiev GP, Iwanaga J, Tubbs RS. The clinical anatomy of variations of the pectoralis minor. Surg Radiol Anat. 2021;43(5):645-651. doi:10.1007/s00276-021-02703-y
9. Lengelé B, Nyssen-Behets C. Anatomical bases for the radiological delineation of lymph node areas. upper limbs, chest and abdomen. Radiother Oncol. 2007;84(3):335-47.
doi: 10.1016/j.radonc.2007.07.016.
10. Iwanaga J, Singh V, Ohtsuka A, et al. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from Anatomical Journal editors. Clin Anat. 2020;34(1):2-4. doi:10.1002/ca.23671